Understanding Pain
Rey Allen & Marie Zahn, Certified Rolfers
During the past twenty years, research on chronic pain has significantly increased, with advances in understanding its etiology, assessment, and treatment (Turk & Monarch 2002; Gatchel 2004, 2005). These discoveries have important healthcare implications as pain is the leading cause for why people seek out medical care, even more so for manual therapy. Whether or not pain relief is your immediate goal, the fact remains that the majority of people who walk into your office experience some degree of pain; as such, we must understand what pain is and most importantly what pain is not.
This article is a review of the most recent understanding of pain, summarizing some of the latest pain science research that is both relevant and applicable to you and your clients. It proposes explanations for phenomena where, with your treatment, some clients’ pain decreases, remains the same, or perhaps gets worse. Most importantly, this understanding is empowering for both you and your clients.
Client expectations and fears play important roles in the outcome—positive and negative—of manual therapy. These expectations of treatment outcomes mainly include pain relief, improved function, and improved overall well-being—including mental well-being. That being said, having a good understanding of the neurobiology of pain will help practitioners meet their client’s personal goals for seeking out care.
Within roughly the last twenty years, neuroscience and pain science has disproven the belief that pain exists solely in the physical tissues, a purely biomechanical explanation for pain (Gifford 1998). This is important; it is a major falsification of what we once believed. The International Association for the Study of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” Simply put, pain is the brain’s perception of tissue damage (Butler & Moseley 2003). Perception is key, because pain is about how a person consciously and non-consciously creates meaning of his/her physical reality. This perception of tissue damage (i.e. pain) is modulated by a number of cognitive, emotional, and sensory inputs (Carlino et al. 2014; Gifford 1998).
When someone in pain walks into your office, they want answers to the following:
1. What’s wrong with me?
2. How long is this going to last?
3. Is there anything I [the client] can do about it?
4. Is there anything you [the practitioner] can do about it? (Verbeek et al. 2004; Gifford 2013)
When considering these questions, they make sense in terms of survival. However, if these questions are left unanswered, we begin to worry about potential disability in the future. When experiencing physical pain we sensibly, but mistakenly, place all of our attention in the physical domain. This leads us to conclude that pain is entirely a reflection of the state of our tissues, assuming the biomechanical model for explaining pain: poor mechanics = pain. Today, we see (this assumption) falsified.
PAIN 101
One of the brain’s chief priorities is to keep us safe and protected. Pain warns us of danger and compels us to take action to relieve and avoid that danger. Thus, (the perception of) pain is dependent on how much danger your brain thinks you’re physically in, not how much you really are in. Our response to pain results in altering the way we sit, stand, and move. Even if there are no problems in the tissues, nerves, or immune system, you can still hurt if your brain thinks that you’re in danger (Butler & Moseley 2003).
One class of sensory receptors called nociceptors were once, incorrectly so, referred to as pain receptors. Nociceptors are receptors that require higher thresholds of stimuli to trigger an action potential, which in turn sends larger, more amplified signals to the central nervous system (CNS). These larger signals serve to get a person’s attention, acting as warning signals. The brain, though, can ignore input from the body, large or small, if the brain is either distracted enough or does not value the incoming messages. Pain is context dependent. A notable example of this is seen with soldiers in the heat of battle who are shot but don’t feel pain until much later, once they are out of the dangerous environment.
Nociception is quantitative (a measurement), not qualitative (meaning). The body’s sensory system simply provides raw data to our CNS. It is our brain which must then interpret it’s meaning. So, while nociception is not an essential part of one's pain experience, it can be a very powerful contributor.

Figure 1: Overlap from repair to adaptation. Adapted from Fig. 3 in Lederman (2015).
One of the most important factors in understanding pain is injury-healing times and its relevancy. (rather awkward sentence here). Wound healing is a complex and dynamic process consisting of four phases: hemostasis, inflammation, proliferation, and remodeling. Typically, most tissues heal within 1-6 months. Soft tissue, such as skin, takes around 10 days to 2 weeks. Deeper soft tissue can take 3-6 months, and depending on the type of deeper tissues, it may take up to a year to regain full tensile strength. Bone takes up to 3-6 months to heal and up to a year to fully remodel (Maxson et al. 2012). Pain is mostly experienced during the inflammatory phase of the healing cycle, where there is a flood of chemicals designed to excite the nervous system and lead to pain; glutamate, aspartate, substance P, adrenaline, cortisol, and cholecystokinin. Pain serves an important role during healing to ensure the process is preserved and to prevent further tissue damage in order to make a full recovery (Lederman 2015; Figure 1). But regardless whether ligaments rupture or the deformation of tissues remain permanent, the phases of healing eventually come to end. Recovery is partly a resolution of inflammation and attenuation of nociceptive excitation.
With acute pain, the aim is to support repair, while with chronic pain, its role is more obscure. One way of understanding acute versus chronic pain is time. The mechanism for pain is the same—the brain interpretation of tissue injury. If after the determinant time for healing is complete but the person’s nervous system has not attenuated, pain becomes chronic.
Unfortunately, many healthcare providers do not clearly communicate or adequately educate clients that all tissues eventually heal and that pain and severity is not positively correlated (Moseley 2003; Louw 2012). Many clients, and some clinicians, wrongly believe that once they are injured, they are always in a state of injury. In other words, their experience with episodic pain is an episodic injury, as seen with the term “re-injury." Current research argues that this is not what is happening and thinking so actually impedes the recovery process, leading to more pain (Butler & Moseley 2003; Lederman 2015).

Figure 2: Overlap between alleviation of symptoms and adaptation represents CNS plasticity associated with recovery of chronic pain. Adapted from Fig. 3 in Lederman (2015).
Probability the most a difficult aspect in understanding pain is that how it is not a sequential or linear process but rather an emergent process of neuronal activity and processes. Ant colonies, schools of fish, flocks of birds, and language are examples of emergent processes. Pain is a substantial sensory and emotional experience that is substantial, modulated by psychological, social and contextual factors (Carlino et al. 2014; Figure 2).
PAIN IS A CONTEXT- DEPENDENT EXPERIENCE
Pain should never be seen as context-free but rather context-dependent. Biopsychosocial (what is this?) research clearly shows that pain is a complex experience that never has a single stimulus. Pain may involve sensory, motor, autonomic, endocrine, immune, cognitive, affective, and behavioral components (Gatchel et al. 2007).
The biopsychosocial model (BPS) for chronic pain is a non-dualistic and integrated approach (Engel 1981). BPS is based on a systems approach as well as a way of understanding the client’s subjective experience as an essential contributor to diagnostic accuracy, health outcomes, and human care (Gifford 1998; Carrió 2004). The biological system (bio-) deals with anatomical, structural, and molecular substrates of disease—the client’s physiology. The psychological system (psycho-) deals with effects of psychodynamic factors like motivation, attitudes, and personality on the experience of and reaction to illness and pain. The social system (-social) examines the cultural, environmental, economic, familial, and social circumstances on the expression and experience of illness and pain (Dogar 2007).
Pain should never be seen as context-free but rather context-dependent. Biopsychosocial research clearly shows pain is a complex experience that never has a single stimulus (Figure 2). Pain may involve any combination of sensory, motor, autonomic, endocrine, immune, cognitive, affective, and behavioral components in producing pain. Pain is filtered through an individual’s genetic composition, prior learning history, current psychological status, and sociocultural influences (Gatchel et al. 2007). Thus, tissue damage can occur in the absence of pain. It helps to see the CNS/brain as the central scrutinizing center, continuously sampling (conscious and non-conscious) from it’s environment, body, and past experiences (Gifford 1998; Figure 2).
Figure 3: Mature Organism Model. Adapted from Fig. 2 in Gifford (1998).
STRESS AND ANXIETY
While stress and anxiety commonly overlap, individually they aren’t the same. Stress is a state of mental, emotional, and/or physical arousal due to demanding and adverse circumstances from the environment. This state of arousal results in an intense focus of attention, which could also serve as a distraction from pain. Stress activates the endogenous opioid system which raises the pain threshold, sometimes called “stress-induced analgesia.” (should a reader know what this is?) Yet, prolonged states of chronic stress set up a feedback loop between pain and stress reactivity (Korte et al. 2005). Conversely, anxiety is defined by worry, apprehension, and anticipation of impending events or future pain, which lowers pain thresholds and results in hyperalgesia (more pain), sometimes called “anxiety-induced hyperalgesia” (Carlino et al. 2014).
Those suffering with chronic pain often have other forms of emotional and physical symptoms: anxiety, stress, depression, loss of appetite, fatigue, insomnia, tension, and fear avoidance (Lunderg 2011). Pain often exacerbates these symptoms resulting in complete debilitation. Just as pain can bring forth emotions, emotions can summon pain (Cervero 2012).
It’s normal to worry about the cause of our pain and to give way to anxiety about future disability or think that something is far worse than it actually is. However, anxiety has a great influence on sustaining and increasing the state of pain and sustaining chronic pain (Eccleston & Crombez 2007).
THE NEUROMATRIX THEORY OF PAIN
The current and widely accepted theory of pain is the neuromatrix theory of pain, developed by Ronald Melzack (2001; Figure 3). The neuromatrix is defined as an anatomical substrate for the widespread neuronal network processes that are sculpted by a multitude of sensory inputs, which describe the “body-self neuromatrix.” The neuromatrix reflects the emergent processes of neuronal activity in the brain. When there are repeated cyclical processes and syntheses of nerve impulses through the neuromatrix, the neuromatrix imparts a particular characteristic pattern, called a neurosignature. Put another way, a neurosignature is a particular neuronal pattern in the neuromatrix (Melzack 2001).

Figure 4: The Neuromatrix Theory of Pain. Adapted from Fig. 1 in Melzack (2001).
The neuromatrix theory of pain purposes that pain is an imprint, or “pain neurosignature,” of nerve impulse patterns upon the body-self neuromatrix. There are many inputs to the brain that can create or later trigger a pain neurosignature, including movement, thoughts, emotions, touch, memories, fear, and visual stimuli—to name a few. Interestingly, the neuromatrix requires no actual sensory input for a person to experience pain, only the activation of a pain neurosignature. Phantom limb pain explains this fact.
The most important component of the neuromatrix theory of pain is recognizing that pain is an output of the brain rather than it being dependent on a response to sensory input (Melzack 2001; Gatchel et al. 2007).
EVIDENCE
Always remember, correlation does not imply causation. A recent systematic review of 33 papers with a total of 3,110 subjects published in the American Society of Neuroradiology (Brinjikji et al. 2015) found absence of pain associated with spine degeneration. The occurrence of disc degeneration in healthy, pain-free individuals ranged from 37% of subjects in their 20s to 96% of those 80 years of age (Table 1). Similarly, 30% of those in their 20s had bulging discs (Brinjikji et al. 2015). MRI findings of degenerative changes in the spine and discs are part of the normal aging process rather than a disease or the cause of pain. The results from Brinjikji et al. (2015) showing 50% of asymptomatic individuals 30-39 years of age have disc degeneration, height loss, or disc bulging suggest that even in young adults, degenerative changes may be incidental and not causally related to presenting symptoms (Brinjikji et al. 2015). It strongly suggests that when degenerative spine findings are observed, it may be normal age-related changes rather than a pathology.
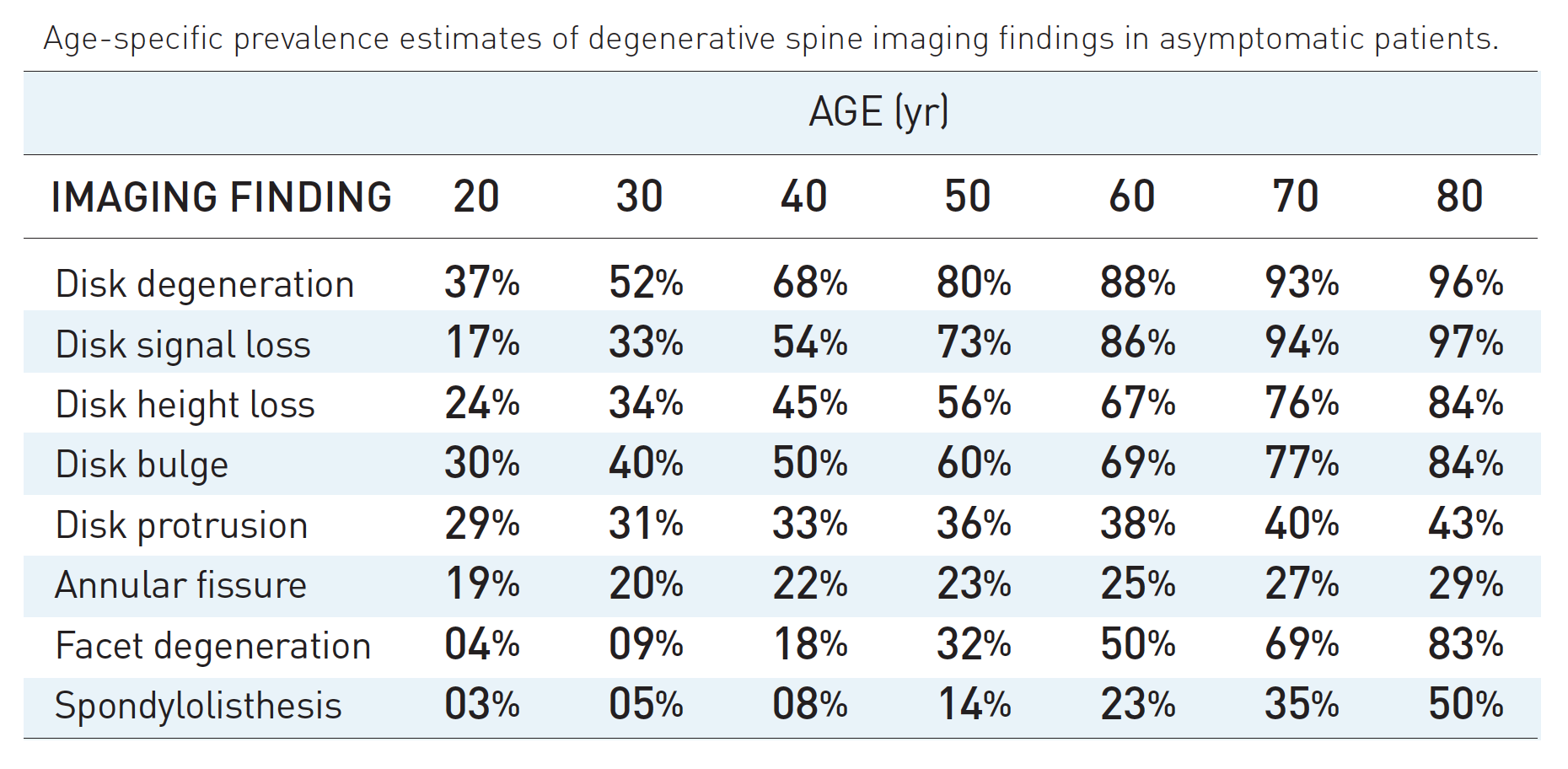
Table 1: Spine images of asymptomatic people. Adapted from Table 2 in Brinjikji et al. (2015)
A study published in Spine (Nakashima et al. 2015) observed MRI findings of cervical spines of 1,211 healthy, asymptomatic Japanese adults between the ages of 20-70. Surprisingly, 73.3% and 78.0% of males and females, respectively, in their 20s had bulging discs, though only 5.3% of all of these asymptomatic subjects were diagnosed with spinal cord compression and increased signal intensity. The conclusion of Nakashima et al. (2015) was that it is dangerous to make interventional decisions based on findings in MRI images alone.
While we believe we’re helping clients by suggesting image testing, what actually takes place is added expenses and increased anxiety surrounding their findings. Both, ironically, can lead to more pain. Consequently, people discontinue their physical activity and restrict living their lives freely. The lesson: it is a grave mistake for our treatment decisions to be based on image findings alone. Hurt does not equal harm.
KNOWLEDGE IS POWER
When a client understands how pain works, they can bring conscious awareness to the triggers of their pain, and in doing so, decrease their pain. Fortunately, change in opinion gives clients more adaptive thoughts and behavior. Research conducted by Louw et al. (2014) showed that giving people a pain education significantly lessens their pain experience post-surgery and reduces medical expenses by 45%. Additionally, Louw et al. (2012) showed that for patients, knowing how a surgical procedure will affect their symptoms is for them the most important. Some practitioners think that their clients cannot understand pain physiology. However, Moseley (2003) showed health professionals inaccurately estimate client’s ability to understand the neurophysiology of pain and that Despite clinicians’ beliefs (I don’t think it’s a good idea to generalize all clinicians this way) that patients aren’t able to understand pain physiology, clients can and want to understand their pain. (Moseley 2003).
Understanding pain gives clients the confidence and self-efficacy in knowing that their bodies are sensitive, not vulnerable or fragile. Self-efficacy for people with chronic pain is when they have the internal resources (confidence) to carry out certain activities or achieve a desired outcome in spite of experiencing pain (Lee et al. 2015). In other words, for a person seeking to engage in a particular behavior or activity, they’re more likely to do that if they feel like they have the internal resources to perform regardless of their pain.
With 172 subjects, Costa et al. (2011) examined whether pain self-efficacy and/or fear of movement mediated the relationship between pain intensity and the disability of pain. What they found was that beliefs of pain self-efficacy and fear of movement partially mediated the effects of pain intensity and disability at the onset of pain. Moreover, 12 months after the onset of low back pain, subjects with high self-efficacy possessed less pain intensity and disability. Additional studies support the relationship between higher patient self-efficacy and lower levels of pain and disability (Reid et. al 2003; Denison et al. 2004; Dohnke et al. 2005). These conclusions were supported in a systematic review and meta-analysis examined by Lee et al. (2015). The study involved 2961 subjects where the research team tested what roles of fear, catastrophization, self-efficacy, and other variables such as psychological distress (depression and anxiety) have in determining disability with people with low back pain and neck pain. While all of these variables interrelate, they found that self-efficacy was the strongest mediator, followed by psychological distress, and then fear of pain. Catastrophizing was not statistically significant as a mediator.
Teaching a person with chronic pain the science of their pain is a cognitive behavioral management tool and treatment target. If done well, it has the potential to reduce client’s fears, which decreases pain intensity and lowers overall disability. Pain education supports the intended goals, in all forms of therapies, in motivating clients to play a more active role in their recovery (Nicholas et al. 1992; Altmaier et al. 1993). That said, this is no easy task. It must be appreciated how deep-seated client’s beliefs are and the preconceived ideas they have of their body. Through a willingness to commit time and effort to properly educate clients, clinicians can have a profound affect in empowering clients to get back to living life more fully (Lederman 2015).
Practice makes perfect. Rehearsing any task results in higher proficiency of that task. This is a rule of neuroplasticity. The same applies if our attention is always focused on our pain, the nervous system, at all levels, will alter itself physically and chemically to be more sensitive. As pain persists, the nervous system becomes better at producing pain. How does this happen? The neurobiology is complicated but here is a short version: the peripheral nervous system (PNS) lays down more ion channels, which causes the nerve signal to be more amplified with smaller input. What previously was considered to be an innocuous stimulus may now read as noxious, making it harder for ordinary CNS inhibitory mechanisms to operate effectively. Danger signals now allowing propagate more signals throughout the nervous systemto flow to the brain uninhibited and amplified, leaving the brain to conclude that there is danger in the tissues , called descending inhibitory pain modulation (Kwon et al. 2014).
CONCLUSIONS
Our experience of pain is a top-down process—always. In fact, there is no such thing as myofascial pain, bone pain, organ pain, or even the existence of nerve pain. There’s just pain. This means damaged and pinched nerves do not have to hurt. Even in the presence of actual tissue damage—given pain is an output of the brain—it is our brain that concludes whether concluding that our tissues are in danger.
Pain is primarily a psychological experience (Craig and Hadjistavropoulos 2004). This is not to say that pain is all in your head, as in your imagination, but it is a construct of the brain. Modern pain science does NOT imply people imagine their pain. Pain is real. Pain is always real. Pain literally changes our PNS and CNS physically and chemically. This is neuroplasticity actually working against us.
Pain Science not only reveals our misunderstanding about how pain works but also examines how our common vernacular as practitioners actually cause more hurt in the end. First, we must be careful not to discount our client's pain experience, even if we think we already have an understanding of their false beliefs. Commonly, clinicians feel rushed to get the educational portion of their treatment over with but this can only serve to further invalidate a client's pain experience. By not alloting time to fully listen to our client's complaints, stories, and values, we run the risk of invalidating their pain and truly misunderstand who they are as a victim of pain (Wernicke 2015). Secondly, we should be mindful of our speech. Are we using terms that incite fear and worry? Additionally, If we refer to pain as an experience (verb) rather than a thing (noun), we signal to our clients that their pain is a state that has the ability to change. This encourages a moreactive enrollment from our clients in their recovery. This also provides insight for them to see that their thoughts and behavior lead to positive or negative consequences. Sadly, referring to pain as a noun misplaces the multi-factorial experience pain is. Pain as a noun also can mislead both practitioners and clients to think pain is in tissues thus can be removed from their tissues (noun). This can only serve to cause more harm. If we're speaking in wrong terms, we're thinking in wrong terms.
Whether in a state of chronic or acute pain, incessant worry, fear avoidance, and self-diagnosing only further sensitizes one’s nervous system. When false beliefs are determined as the root of causing harm, providing client education is one of the most effective interventions. At the same time, we don’t want to cause too much cognitive dissonance at first when explaining pain. We must take special care when educating clients who seem to use their pain to self-identify.
Above all, explain pain on purpose!
TIPS:
- First, listen to your clients and their stories and make sure that they know you care. Surprisingly, we’ve seen that the strongest factor linked to client’s improvement is not the thoroughness of the medical history or physical assessment—tests ordered or drugs prescribed. The single most important factor is whether or not clients indicated that the doctor had carefully listened to their descriptions of their condition on the first visit.
- Provide reassurance that they and their body’s tissue is ok, because tissues are resilient. Remember, all tissues heal.
- Correct any false beliefs you hear coming from the client throughout treatment about pain, as this is a paradigm shift for most people. Know that not everyone will get it at first, so be kind, be patient, and be persistent. Encourage clients to police their thoughts of worry and to make it a point to laugh more.
- Don’t let “pain be your guide.” This leads to fear-avoidant behavior, causing pain to persist in the long-term. Hurt doesn’t equal harm. It equals habit.
- Strongly suggest that they have an exercise regime that matches their tolerances, grading their exposure. Exercise is analgesia and builds client’s confidence in their tissues (Gurevich et al. 1994). Refer to a physio or personal trainer who is updated with pain science so that the message is confirmed and consistent.
- Encourage clients to strengthen their social network and to seek out fun and laughter.
- Have in your rolodex the contact of a pain therapist to refer to for a more thorough pain education. It’s best when this information comes from multiple sources.
- Build self-efficacy!
“Following injury, or any noxious event, people’s feelings or emotions and thoughts about their situation will change. Injury and the consequent of pain may produce powerful aversive feelings of fear, anxiety or increasing anger.” -Louis Gifford
“Pain is an opinion on the organism’s state of health rather than a mere reflexive response to injury. The brain gathers evidence from many sources before triggering pain.” -V.S. Ramachandran
“To reduce pain, we need to reduce credible evidence of danger and increase credible evidence of safety.” –Lorimer Mosely
“Think about it: A patient comes to you seeking help for pain, and you teach the patient anatomy! No wonder pain rates in the US have doubled in the last 15 years alone. Never before have we performed as much surgery or prescribed as much medicine for pain in the history of mankind, and pain rates are ever increasing.” -Adriaan Louw, PT, PhD
“Don’t move the way fear makes you move.” –Rumi
REFERENCES
Altmaier E.M., D.W. Russel, C.F. Kao, T.R. Lehmann, J.N. Weinstein(1993). Role of self-efficacy in rehabilitation outcome among chronic low back pain patients. Journal of Counsel Psychology, 40: 335-339.
Brinjikji W., Luetmer, P. H., Comstock, B., et al. (2015). Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. AJNR. American Journal of Neuroradiology, 36(4): 811–816.
Butler D., T. Cocks (2015). Noinotes: DIM SIMs.
Butler D., L Moseley (2003). Explain Pain. Adelaide, Australia, Noigroup pub. Print.
Carlino E., E. Frisaldi, F. Benedetti (2014) Pain and the context. Nat. Rev. Rheumatol, 10: 348–355.
Cervero F. (2012). Understanding Pain. Massachusetts: The MIT Press.
Carrio F.B., A. Suchman, R. Epstein (2004). The Biopsychosocial Model 25 Years Later: Principles, Practice, and Scientific Inquiry. Annals of Family Medicine, 2(6): 576–582.
Costa L., C. Maher, J. McAuley et al. (2010). Self-efficacy is more important than fear of movement in mediating the relationship between pain and disability in chronic low back pain. European Journal of Pain, 15(2): 213-219.
Craig K., T. Hadjistavropoulos (2004). Pain: Psychological Perspectives. Mahwah, New Jersey: Lawrence Erlbaum Assoc. Print.
Denison E., P. Asenlof, P. Lindberg, E. Denison (2004). Self-efficacy, fear avoidance, and pain intensity as predictors of disability in subacute and chronic musculoskeletal pain patients in primary health care. Pain, 111:245-252.
Dogar I.A. (2007). Biopsychosocial model. Annals of Punjab Medical College, 1(1): 11-13.
Dohnke B., B. Knäuper, W. Müller-Fahrnow (2005). Perceived self-efficacy gained from, and health effects of, a rehabilitation program after hip joint replacement. Arthritis Care Res, 53: 585-592.
Eccleston C., G Crombez (2007). Worry and chronic pain: A misdirected problem solving model. Pain, 132: 233–236.
Engel G.L. (1981). The clinical application of the biopsychosocial model. The Journal of Medicine and Philosology, 6 (2): 101-124.
Gatchel R. J. (2004b). Comorbidity of chronic pain and mental health: The biopsychosocial perspective. American Psychologist, 59: 792–794.
Gatchel R. J., Y Peng, M. Peters, P. Fuchs, D. Turk. (2007) The Biopsychosocial Approach to Chronic Pain: scientific advances and future directions. Psychological bulletin, 133.4: 581-624.
Gifford L, (1998). Pain, the tissues and the nervous system: a conceptual model. Physiotherapy, 84 (1).
Gifford L, (2014). Aches and Pains. book 1 of 3, section 10. Dalmouth, Cornwall, CNS Press. Print.
Gurevich M., PM. Kohn, C. Davis. (1994). Exercise-induced analgesia and the role of reactivity in pain sensitivity. J Sports Sci., 12(6):549-59.
Hardy M. (1989). The Biology of Scar Formation. PHYS THER., 69:1014-1024.
Hsu C. et. al. (2014). New perspectives on patient expectations of treatment outcomes: results from qualitative interviews with patients seeking complementary and alternative medicine treatments for chronic low back pain. BMC Complementary and Alternative Medicine, 14:276.
Korte S. M., Koolhaas, J. M., Wingfield, J. C., McEwen, B. S. (2005). The Darwinian concept of stress: Benefits of allostasis and costs of allostatic load and the trade-offs in health and disease. Neuroscience and Bio-behavioral Reviews, 29, 3–38.
Kwon M., M. Altin, H. Duenas, L. Alev. (2014). The role of descending inhibitory pathways on chronic pain modulation and clinical implications. Pain Practice, 14 (7) :656-67
Lederman E. (2015). A process approach in manual and physical therapies: beyond the structural model. CPDO Online Journal, p1-18.
Lee H., M. Hubscher, G. L. Moseley et al. (2015). How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain journal, 156: 988–997.
Louw A., D. Butler, I. Diener, E. Puentedura (2012). Preoperative education for lumbar radiculopathy: A survey of US spine surgeons. Int J Spine Surg., 1 (6): 130-9.
Louw A, Diener I., Landers M.R., Puentedura E.J. (2014). Preoperative pain neuroscience education for lumbar radiculopathy: a multicenter randomized controlled trial with 1-year follow-up. Spine, 39(18):1449-57.
Louw A., E. Puentedura (2013). Therapeutic neruoscience education, teaching patients about pain. USA: International Spine and Pain Institute. Print.
Lunderg M., A. Grimby-Ekman, J. Verbunt, M.J. Simmonds (2011). Pain-Related Fear: A Critical Review of the Related Measures. Pain Research and treatment, article id 494196.
Maxson S., E. Lopez, D. Yoo, MA. Leroux, et al. (2012) Concise review: role of mesenchymal stem cells in wound repair. Stem Cells Transl. Med., 1(2):142-9.
Melzack R. (2001). Pain and the Neuromatrix in the Brain. Journal of Dental Education, 65(12): 1378-1382.
Moseley L. (2003). Unraveling the barriers to reconceptualization of the problem in chronic pain: The actual and perceived ability of patients and health professionals to understand the neurophysiology. Journal of Pain 4(4):184-189.
Nakashima H., Y. Yukawa, K. Suda, M. Yamagata, T. Ueta, F. Kato. (2015). Abnormal findings on magnetic resonance images of the cervical spines in 1211 asymptomatic subjects. Spine, 40(6):392-8.
Nicholas MK. (1989). Self-efficacy and chronic pain. In: Paper presented at the annual conference of the British psychological society, St. Andrews, Scotland.
Reid M.C., C.S. Williams, T.M. Gill (2003). The relationship between psychological factors and disabling musculoskeletal pain in community-dwelling older persons. Journal of the American Geriatrics Society, 51(8):1092-1098.
Turk D. C., & Monarch, E. S. (2002). Biopsychosocial perspective on chronic pain. In D. C. Turk & R. J. Gatchel (Ed.), Psychological approaches to pain management: A practitioner’s handbook (2nd ed., pp. 3–30). New York: Guilford Press.
Verbeek, J., Sengers, M. J., Riemens, L., & Haafkens, J. (2004). Patient expectations of treatment for back pain: a systematic review of qualitative and quantitative studies. Spine, 29(20), 2309-2318.
Wernicke S., J. Huberts, P. Wippert (2015). The pain of being misunderstood: Invalidation of pain complaints in chronic. Journal of Health Psychology, 1–13.